
What’s new with Anaphylaxis? (5 min read)
In this week’s blog we’ll be talking about what’s new in the Resus 2021 Anaphylaxis guideline as this is the one probably with the most changes and topical with exams due to the recent guidance as well as the most recent NAP 6 project!
Your initial assessment and simultaneous management remains the same.
So ALWAYS…
1. Call for Help!
2. Declare a critical incident
3. And proceed with your ABCDE assessment, ensuring the patient has 100% O2 applied!
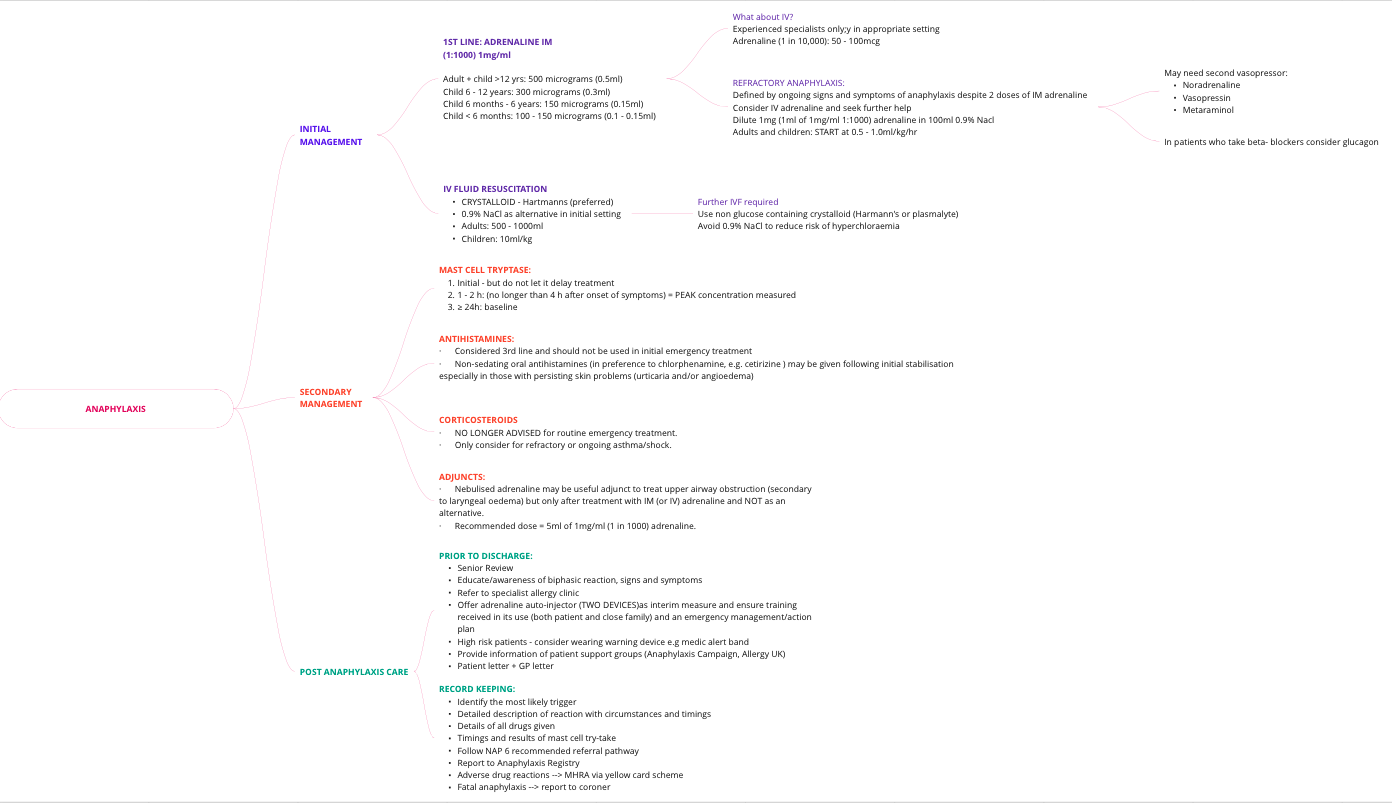
Lets start with the main CURRENT recommendations:
Now for some definitions:
Anaphylaxis:
Serious systemic life threatening hypersensitivity reaction that is usually rapid in onset.
Refractory anaphylaxis
anaphylaxis requiring ongoing treatment (due to persisting CVS/Resp symptoms) despite TWO appropriate doses of IM adrenaline
Pathophysiology:
The pathophysiology is poorly understood but may be due to:
- Delayed or insufficient delivery (common)
- Progression due to ongoing release of inflammatory mediators (common)
- Tachyphylaxis (uncommon)
The May 2021 guidance includes an excellent diagram summarising the main physiological changes:
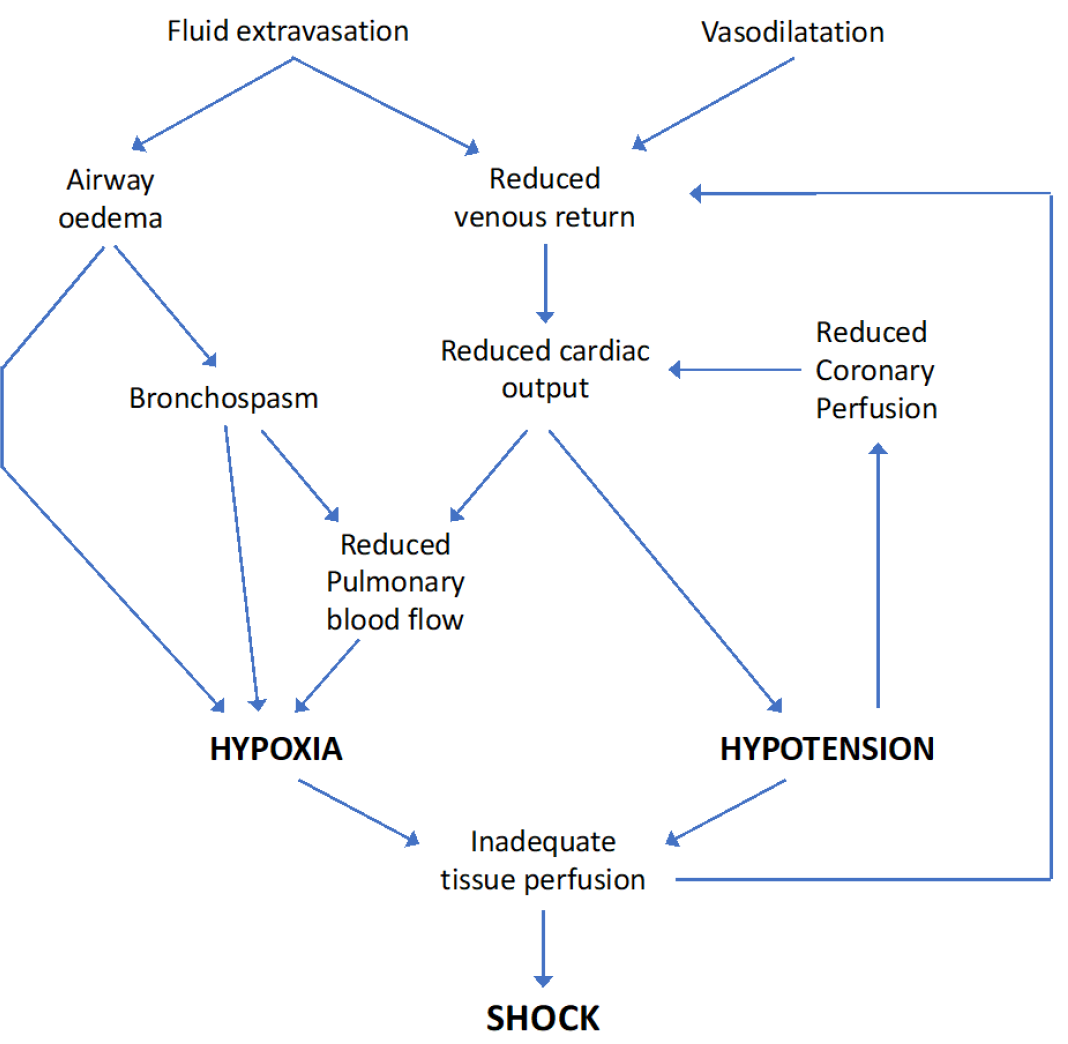
Physiological mechanisms responsible for anaphylactic shock
Grading of hypersensitivity reactions
5 grades:
Grade 1 - cutaneous features = rash, itch, swelling
Grade 2 – mild hypotension and wheeze (mild) +/- Grade 1
Grade 3 – severe features opf teha bove +/- airway swelling
Grade 4 – Requires CPR
Grade 5 – death
Grade 1 – 2: mild – moderate
Grade 3 – 5: hypersensitivity may be termed anaphylaxis
Why is it important to anaesthetists?
NAP 6 revealed the following biggest contributors to anaphylaxis in perioperative medicine and these are drugs we use extremely freeuqnetly so vigilance is a must!
Commonest PERIOPERATIVE triggers:
1. Antibiotics
a. Of which co-amoxiclav (23%) and teicloplanin (18%) are the biggest contributors
2. Neuromuscular blocking agents
3. Chlorhexidine
4. Patent blue dye
Food allergies to be aware of, particularly if you get called to ED in an emergency:
Commonest triggers:
1. Peanuts
2. Tree nuts
3. Cows milk (children)
A note on adrenaline infusions:
Dilute 1mg (1ml of 1mg/ml 1:1000) adrenaline in 100ml 0.9% Nacl
Start at 0.5 – 1.0ml/kg/h in adults and children
Titrate accordingly
Steady state reached in 5 – 10 mins
What are the signs of excessive adrenaline treatment?
Tachycardia, tremor, pallor with a normal or raised BP
How do you wean adrenaline infusions?
Ensure specialist/senior help is available
As symptoms improve, reduce by 50% of the starting rate
Progressively reduce over 30 minutes to stop, one hour after resolution of all symptoms and signs
Top Tips from NAP 6:
Do not give test doses - they project the same risk as severity is not linked to quantity given
Obstetrics – NAP 6 found that in anaphylaxis adrenaline administered was less and phenylephrine more - the concern about adrenaline impact on uteroplacental blood flow is unfounded
References:
https://www.resus.org.uk/sites/default/files/2021-05/Emergency%20Treatment%20of%20Anaphylaxis%20May%202021_0.pdf
https://www.resus.org.uk/library/2021-resuscitation-guidelines/executive-summary-main-changes-2015-guidelines
https://www.resus.org.uk/sites/default/files/2021-04/Anaphylaxis%20Summary%20Document.pdf
https://www.nationalauditprojects.org.uk/NAP6Report?newsid=1914