
A brief introduction to the Vortex approach (5 min read)
The Vortex Approach is recognised as a ‘high acuity implementation tool,’ designed to complement algorithms you may be used to published by the Difficult Airway Society.
One of the key differences in which the Vortex Approach may help you in your day-to-day practice is by helping to simplify decision making when it comes to airway management.
The prime focus is on ensuring alveolar oxygen delivery and the variety of ways in which this can be done.
Background:
It can be difficult to remember algorithms, particularly in highly pressurised situations.
Instead of a linear approach to airway management, the vortex approach is more lateral in that airway management can start at any point and change according to clinician judgement. Users of the Vortex Approach are able to move from one airway technique to another if this is deemed as the most appropriate way to optimise and deliver alveolar oxygenation.
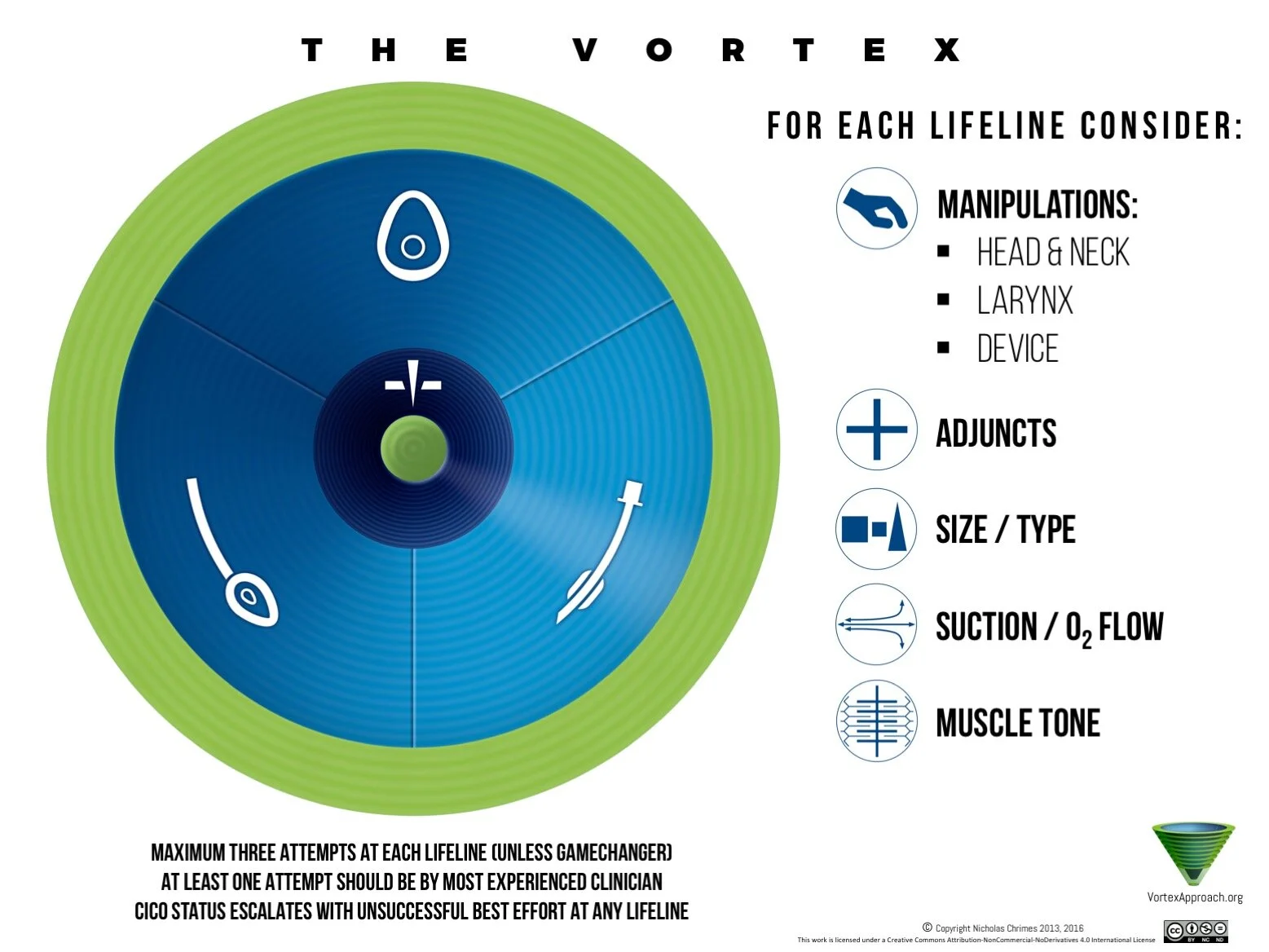
This is demonstrated by the following circular arrangement known as THE VORTEX
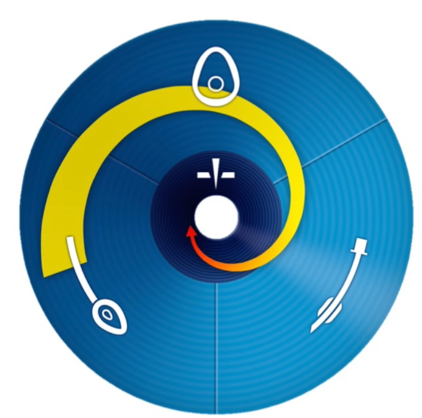
Potential sequence of best efforts commencing with a supraglottic airway

Potential sequence of best efforts commencing with endotracheal tube
The “ZONES”
Green zone:
=Confirmation of alveolar oxygen delivery; opportunity to:
re-oxygenate
gather resources
develop a strategy if a patient has still not got an established airway.
The green zone is present as an outward ring when any of the 3 upper airway techniques aid in delivering alveolar oxygen delivery and also in the inward centre, when emergency front-of-neck access secures alveolar oxygen delivery.
Blue zone:
=There are 3 upper airway (non-surgical) techniques known as ‘LIFELINES,’ by which alveolar oxygen delivery can be established and confirmed:
Face mask
Supraglottic device
Endotracheal tube
Dark blue zone:
= represents potential for worsening hypoxaemia and cyanosis if alveolar oxygenation is not restored urgently.
A maximum of 3 attempts at each lifeline is recommended with at least one attempt by the most experienced clinician
Best efforts:
If a ‘best effort’ at each of these 3 lifelines is attempted then a Can’t Intubate, Cant Oxygenate (CICO) situation is declared and emergency front-of-neck access must be initiated.
A best effort is deemed by 5 categories of optimisation and applies to all 3 upper airway lifelines, again making supportive decision making somewhat more standardised and easier.
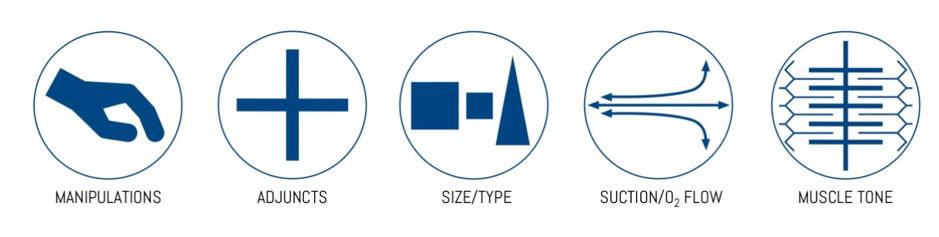
The 5 categories have the following easily recognisable ‘icons’
Completion of a ‘best effort’ without being able to establish or restore alveolar oxygen delivery moves you in a spiral movement inwards towards the next lifeline, and closer to the CICO lifeline.
Additions to the Vortex Approach
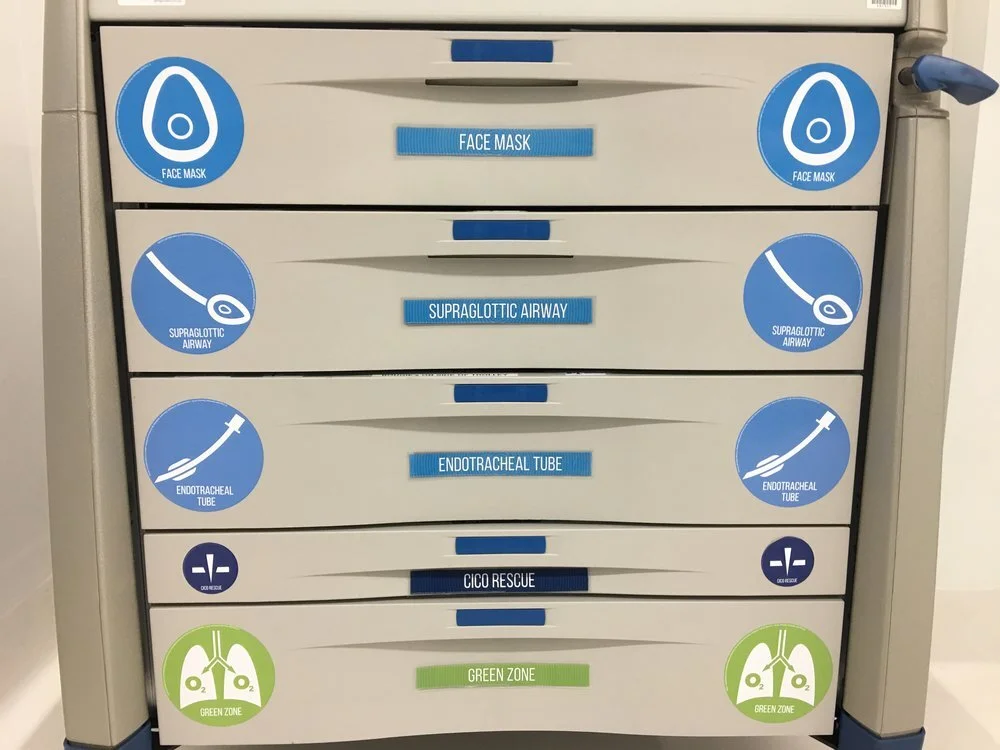
The Vortex Approach is also implemented in practice by some hospitals having the Vortex Airway Rescue Cart. The airway rescue cart is laid out in order of lifelines, and includes only immediately necessary equipment.
It also contains “prompt” cues for non-equipment interventions.
These trolleys would be similar to ‘difficult airway trolleys’ you may be used to.
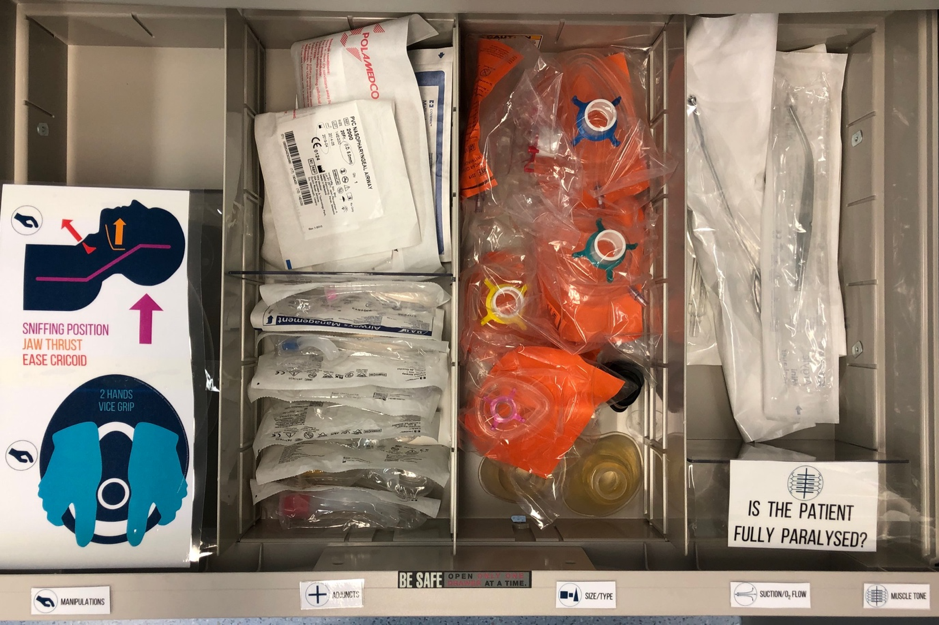
An example of a face mask drawer layout
Benefits to using the Vortex approach:
- Can be used to plan day-to-day airway management, encouraging you to think about what you would do if your plan A did not work in the particular situation?
- Facilitates efficient best efforts at each of the 3 upper airway lifelines
- Encourages thoughtful and appropriate decision making when “green zone” is entered
- Promotes early recognition of a potential CICO situation as lifelines are exhausted and one heads down the circumferential inward movement of the vortex.
- The Vortex Airway Rescue cart means that other members of the team may also be prompted to make suggestions, therefore reducing cognitive load, and helping to aid in decision making.
- Complimenting the Vortex approach with the Vortex Airway Rescue Cart improves the ability of clinicians to easily locate required devices.
- The Vortex Approach is a simple mental model to complement Difficult Airway Society guidelines and algorithms.
Remember this is a useful implementation tool, and is NOT designed to replace Difficult Airway Society (DAS) algorithms.
If you’re sitting the exam – the DAS algorithms are the correct textbook answers!
Further information:
The Vortex Approach website explains things in more details, contains useful videos to help you understand the Vortex Approach further and also has an interesting video re-creating the Elaine Bromley case
http://vortexapproach.org