
Resuscitation: Special circumstances part 1 of 2 (8 - 10 min read)
Drowning and Hypothermia
With the return of face to face exams coming up imminently, I wonder what resuscitation scenario’s the college will get you all to act out. I’ve created a 2 part series focusing on special circumstances in resuscitation so you don’t find yourselves caught out!
In this blog post we’ll cover the following:
Basic definitions
Key points
Causes of drowning
Pathophysiology of drowning
Management of drowning and hypothermia: Pre hospital —> hospital
Hypothermia
Hypothermia ALS guidance
Methods of rewarming
Management of drowning and hypothermia: In hospital goals
Summary
Let’s get cracking!
————————————————
Definitions:
Drowning: Drowning is the process of experiencing respiratory impairment from submersion/immersion in liquid (WHO 2002 definition)
Immersion: airway is ABOVE the surface of the liquid (e.g. having a bath, surfing)
Submersion: airway is BELOW the surface of the liquid
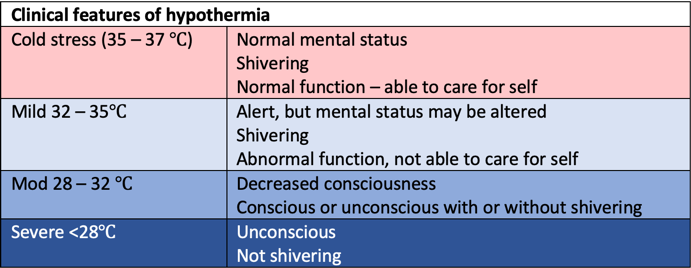
Hypothermia classification: (varies slightly from textbooks)
Mild 32 – 35 degrees centigrade
Mod 28 – 32 degrees centigrade
Severe <28 degrees centigrade
2. Key points:
· Submersion duration is the strongest predictor of outcome
· Prognosis determined by severity and duration of cerebral hypoxia/anoxia and the amount of water than that has been aspirated
· Hypothermia and drowning is associated with a protective mechanism that potentially increases survival rate
o How? – rate of CMRO2 reduced by approx. 5-7% for each reduction of 1°C in temperature within the range of 37°C to 20°C
· These patients often require prolonged resuscitation attempts as per the hypothermia resuscitation guidance (see below)
3. Causes of drowning:
Misadventure
Inadequate supervision of small children
Neurological event e.g. epilepsy, stroke
Cardiac event e.g., MI, HCM, dysrhythmia, long QT, short QT
Impaired judgement e.g. intoxication
Trauma
Overdose
Foul play
4. Pathophysiology of drowning
Water enters the mouth —>
1. First: voluntarily spat out or swallowed
2. Second: Conscious response to hold breath, until no longer able to
3. Then:
a. Water aspirated into airways —>coughing (reflex response)
b. Continued aspiration à progressive hypoxaemia —> loss of consciousness and apnoea
i. Laryngospasm may also occur
c. Hypoxaemia —> tachycardia —> bradycardia —> PEA —> Asystole
Process usually occurs in seconds to minutes
>1 hour in unusual cases of hypothermia
5. Management of drowning and hypothermia: Pre hospital —> hospital
NB: Only trained individuals should attempt in-water rescue. Otherwise…
Simultaneously assess and manage…
Lift patient out horizontal + attempt to rewarm/minimise heat loss + arrange fast transfer asap…
Remove wet clothing
Wrap in thick blankets
Assess consciousness
Conscious and/or breathing normally —> ABCDE assessment + aim to prevent cardiac arrest
100% oxygen until Spo2 can be measured reliably or ABG obtained
Targets: 94 – 95%, Pao2 10 – 13kpa
Hypothermic + RF for imminent cardiac arrest —> ideally transfer to ECMO centre
Unconscious and not breathing normally —> start resuscitation (ALS algorithm)
Initiate hypothermia algorithm if core temp <35
5 rescue breaths/ventilations with 100% o2 if available
Remains unconscious? Start CPR 30:2 (adult ALS algorithm)
Defibrillate if indicated and available
Early intubation advised
Consider ECPR
6. Hypothermia
Key interventions:
1. Pre-hospital insulation/rewarming
2. Triage
3. Fast transfer
RF for imminent cardiac arrest:
1. Core temperature < 30°C
2. Ventricular arrhythmia
3. SBP < 90 mmHg
7. Hypothermia ALS guidance: Key points:
1. REWARM – unlikely to respond to drugs before warmed
2. <30 - No drugs
3. 30 – 35 - DOUBLE interval between drugs
4. Defibrillation is less effective
o <30 Shockable rhythm? —> 3 stacked shocks, then delay further attempts until >30°C
Prehospital:
· Individuals at risk of cardiac arrest/in cardiac arrest should ideally be directly transferred to an extracorporeal life support (ECLS) centre for rewarming.
8. Methods of rewarming:
Passive rewarming:
Remove wet clothes
Insulate with blankets
Active rewarming:
Peripheral (forced air warmer (bair hugger), hot water bottles)
Central (warmed humidified inspired gases, warmed IVF, lavage, intravascular thermal regulation via vascath, haemofiltration, cardiopulmonary bypass)
Non eCLS (extra-corporeal life support) rewarming should be initiated in peripheral hospital if an ECLS centre cannot be reached within 6 hours
Hypothermic cardiac arrest - rewarming should be performed with ECLS, preferably with ECMO over CPB.
9. Management of drowning and hypothermia: In hospital goals
Continue ABCDE management à likely will require ICU care
Rewarm to 34 for 24 hrs
· Management of organ injury – the following list is not exhaustive but is designed to highlight the key points of care…
AIRWAY: intubate early if indicated
RESP: lung protective ventilation. Risk of ALI and ARDS
CARDIOVASCULAR: < 28 VF is common, SIRS, hypovolaemia from endothelial disruption/cold diuresis
CNS: prevent secondary brain injury - neuroprotective strategies, manage seizures
GI: NG to decompress stomach
RENAL: Risk of rhabdomyolysis, AKI.
METABOLIC: severe metabolic acidosis from raised lactate. Caution PaO2 in cold patient is much lower than the measured value
INFECTION: consider antibiotics if patient submerged in grossly contaminated water
10. Summary
Hopefully by the end of reading this, you’re now able to recognise the links between drowning and hypothermia and appreciate the differences between hypothermic cardiac arrests and your standard ALS cardiac arrest algorithm. Comments welcomed below!
Stay tuned next week for more on resuscitation special circumstances…